Canalicular adenoma
This article may be too technical for most readers to understand. (July 2020) |
Canalicular adenoma is a benign, epithelial salivary gland neoplasm arranged in interconnecting cords of columnar cells. This is a very rare benign neoplasm, that makes up about 1% of all salivary gland tumors, or about 4% of all benign salivary gland tumors.[1][2]
Presentation[]
Most patients present in the 7th decade of life, with females affected much more commonly than males (about a 4:1 ratio). The vast majority of the tumors present in the upper lip, although a few present in the palate or buccal (cheek) tissue as a slowly enlarging mass.[3] It is curious that the tumor may show multifocality or multinodularity, a finding that should not be confused with invasion clinically or with malignancy.[1][4]
Diagnosis[]
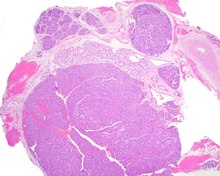
Tumors are usually small because they come to clinical attention early on in development, with an average size of about 1.6 cm.[1] There is a very characteristic appearance to the tumor when reviewed histologically.

There is a canalicular pattern with cords and ribbons showing connection points between opposing columnar cells within spaces that is called a "string of pearls" appearance.

There are often small luminal squamous balls or morules. There is a very well developed supporting tissue that is a loose, fibrillar stroma, rich in hyaluronic acid and chondroitin sulphate.[1] In a few cases small calcifications or microliths may be present. Although seldom necessary, a pathologist can do immunohistochemistry studies to confirm the diagnosis, with the cells strongly reactive with pancytokeratin, S100 protein and SOX10, with a delicate GFAP reaction around the periphery.[5][1][6][7] Even though it is a benign tumor, it must be separated from a basal cell adenoma, pleomorphic adenoma, adenoid cystic carcinoma, and polymorphous adenocarcinoma.
Treatment[]
Recurrences are probably more likely to represent multifocal tumors, with conservative surgery the treatment of choice.[1]
References[]
- ^ a b c d e f Thompson LD, Bauer JL, Chiosea S, McHugh JB, Seethala RR, Miettinen M, Müller S (Jun 2015). "Canalicular adenoma: a clinicopathologic and immunohistochemical analysis of 67 cases with a review of the literature". Head Neck Pathol. 9 (2): 181–195. doi:10.1007/s12105-014-0560-6. PMC 4424207. PMID 25141970.
- ^ Nelson JF, Jacoway JR (Jun 1973). "Monomorphic adenoma (canalicular type). Report of 29 cases". Cancer. 31 (6): 1511–1513. doi:10.1002/1097-0142(197306)31:6<1511::aid-cncr2820310630>3.0.co;2-o. PMID 4709966.
- ^ Suarez P, Hammond HL, Luna MA, Stimson PG (Aug 1998). "Palatal canalicular adenoma: report of 12 cases and review of the literature". Ann Diagn Pathol. 2 (4): 224–228. doi:10.1016/s1092-9134(98)80011-7. PMID 9845742.
- ^ Penner CR, Thompson LD (Mar 2005). "Canalicular adenoma". Ear Nose Throat J. 84 (3): 132. doi:10.1177/014556130508400306. PMID 15871577.
- ^ Ferreiro JA (Dec 1994). "Immunohistochemical analysis of salivary gland canalicular adenoma". Oral Surg Oral Med Oral Pathol. 78 (6): 761–765. doi:10.1016/0030-4220(94)90093-0. PMID 7534898.
- ^ Huebner TA, Almubarak H, Drachenberg CB, Papadimitriou JC (Apr 2014). "Canalicular adenoma--search for the cell of origin: ultrastructural and immunohistochemical analysis of 7 cases and review of the literature". Ultrastruct Pathol. 38 (2): 74–82. doi:10.3109/01913123.2013.833564. PMID 24144157.
- ^ Curran AE, Allen CM, Beck FM, Damm DD, Murrah VA (Sep 2007). "Distinctive pattern of glial fibrillary acidic protein immunoreactivity useful in distinguishing fragmented pleomorphic adenoma, canalicular adenoma and polymorphous low grade adenocarcinoma of minor salivary glands". Head Neck Pathol. 1 (1): 27–32. doi:10.1007/s12105-007-0003-8. PMC 2807497. PMID 20614277.
- Oral neoplasia