Tennis elbow
| Tennis elbow | |
|---|---|
| Other names | Lateral epicondylalgia, lateral elbow tendinopathy[1] |
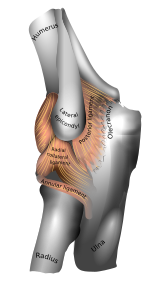 | |
| Left elbow-joint, showing posterior and radial collateral ligaments. (Lateral epicondyle visible at center.) | |
| Specialty | Orthopedics, sports medicine |
| Symptoms | Painful and tender outer part of the elbow[1] |
| Usual onset | Gradual[2] |
| Duration | Less than 1 to 2 years[3] |
| Causes | Excessive use of the muscles of the back of the forearm[2] |
| Risk factors | Smoking, obesity[3] |
| Diagnostic method | Based on symptoms with medical imaging used to rule out other potential causes[2] |
| Differential diagnosis | Osteochondritis dissecans, osteoarthritis, radiculopathy[3] |
| Treatment | Changing activities, physical therapy, pain medication[1] |
| Frequency | c. 2%[3] |
Tennis elbow, also known as lateral epicondylitis, is a condition in which the outer part of the elbow becomes painful and tender.[1] The pain may also extend into the back of the forearm and grip strength may be weak.[2][1] Onset of symptoms is generally gradual.[2] Golfer's elbow is a similar condition that affects the inside of the elbow.[1]
It is due to excessive use of the muscles of the back of the forearm.[2] Typically this occurs as a result of over use during work or sports, classically racquet sports.[1][2] The diagnosis is typically based on the symptoms with medical imaging used to rule out other potential causes.[2] It is more likely if pain increases when a subject tries to bend back the wrist when the wrist is held in a neutral position.[1] A powered screwdriver can cause this injury if overused one-handed. It is classified as a chronic tendinosis, not a tendinitis.[1]
Treatment involves decreasing activities that bring on the symptoms together with physical therapy or other treatment gradually increasing loads.[4][1] Pain medications such as NSAIDS or acetaminophen (paracetamol) may be used.[1] A brace over the upper forearm may also be helpful.[2] If the condition does not improve corticosteroid injections or surgery may be recommended[1] although some experts recommend avoiding cortisone injections due to poor long-term results in high-quality trials.[5][6][7][8] Many people get better within one month to two years.[3][9]
About 2% of people are affected.[3] Those 30 to 50 years old are most commonly affected.[2] The condition was initially described in 1873.[3] The name "lawn tennis elbow" first came into use for the condition in 1882.[10]
Signs and symptoms[]
- Pain on the outer part of the elbow (lateral epicondyle)
- Point tenderness over the lateral epicondyle—a prominent part of the bone on the outside of the elbow
- Pain from gripping and movements of the wrist, especially wrist extension (e.g. turning a screwdriver) and lifting movements[11]
Symptoms associated with tennis elbow include, but are not limited to, radiating pain from the outside of the elbow to the forearm and wrist, pain during extension of wrist, weakness of the forearm, a painful grip while shaking hands or torquing a doorknob, and not being able to hold relatively heavy items in the hand.[12] The pain is similar to the condition known as golfer's elbow, but the latter occurs at the medial side of the elbow.[13]
Terminology[]
The term "tennis elbow" is widely used (although informal), but the condition should be understood as not limited to tennis players.[14][15] Historically, the medical term "lateral epicondylitis" was most commonly used for the condition.[2][14][15][16]
Since histological findings reveal noninflammatory tissue, the term “lateral elbow tendinopathy," "tendinosis,” or “angio-fibroblastic tendinosis” have been suggested instead of “lateral epicondylitis”.[17][18] Most recently, in 2019, a group of international experts agreed that "lateral elbow tendinopathy" was the most appropriate terminology.[19]
Causes[]

Tennis elbow is a type of repetitive strain injury resulting from tendon overuse and failed healing of the tendon. In addition, the extensor carpi radialis brevis muscle plays a key role.[18][20]

Early experiments suggested that tennis elbow was primarily caused by overexertion. However, studies show that trauma such as direct blows to the epicondyle, a sudden forceful pull, or forceful extension cause more than half of these injuries.[21] Repeatedly mis-hitting a tennis ball in the early stages of learning the sport causes shock to the elbow joint and may contribute to contracting the condition.[22]
There are multiple aspects of tennis that may cause a player to develop “tennis elbow”. From a technical perspective, leading a backhand with your elbow, excessive pronation of the forearm when putting topspin on a forehand, and excessive flexion of the wrist on a serve can all greatly lead to tennis elbow. Other things that can be improved are: racquet type, grip size, string tension, type of court surface, and ball weight.[23]
Pathophysiology[]
Histological findings include granulation tissue, micro-rupture, degenerative changes, and there is no traditional inflammation.[18][24][9]
Longitudinal sonogram of the lateral elbow displays thickening and heterogeneity of the common extensor tendon that is consistent with tendinosis, as the ultrasound reveals calcifications, intrasubstance tears, and marked irregularity of the lateral epicondyle. Although the term “epicondylitis” is frequently used to describe this disorder, most histopathologic findings of studies have displayed no evidence of an acute, or a chronic inflammatory process. Histologic studies have demonstrated that this condition is the result of tendon degeneration, which replaces normal tissue with a disorganized arrangement of collagen. Therefore, the disorder is more appropriately referred to as tendinosis or tendinopathy rather than tendinitis.[17]
Colour Doppler ultrasound reveals structural tendon changes, with vascularity and hypo-echoic areas that correspond to the areas of pain in the extensor origin.[25]
The pathophysiology of lateral epicondylitis is degenerative. Non-inflammatory, chronic degenerative changes of the origin of the extensor carpi radialis brevis (ECRB) muscle are identified in surgical pathology specimens.[26] It is unclear if the pathology is affected by prior injection of corticosteroid.[citation needed]
Tennis players generally believe tennis elbow is caused by the repetitive nature of hitting thousands of tennis balls, which leads to tiny tears in the forearm tendon attachment at the elbow.[16]
The extensor digiti minimi also has a small origin site medial to the elbow that this condition can affect. The muscle involves the extension of the little finger and some extension of the wrist allowing for adaption to "snap" or flick the wrist—usually associated with a racquet swing. Most often, the extensor muscles become painful due to tendon breakdown from over-extension. Improper form or movement allows for power in a swing to rotate through and around the wrist—creating a moment on that joint instead of the elbow joint or rotator cuff. This moment causes pressure to build impact forces to act on the tendon causing irritation and inflammation.[citation needed]
At least one author questions that lateral epicondylitis is caused by repetitive microtrauma/overuse, maintaining the theory is likely overstated and lacks scientific support.[26]
Other speculative risk factors for lateral epicondylitis include taking up tennis later in life, unaccustomed strenuous activity, decreased mental chronometry and speed and repetitive eccentric contraction of muscle (controlled lengthening of a muscle group).[citation needed]
Diagnosis[]
Physical examination[]
To diagnose tennis elbow, physicians perform a battery of tests in which they place pressure on the affected area while asking the patient to move the elbow, wrist, and fingers. Diagnosis is made by clinical signs and symptoms that are discrete and characteristic. For example, when the elbow fully extended, the patient feels points of tenderness over the affected point on the elbow. The most common location of tenderness is at the origin of the extensor carpi radialis brevis muscle from the lateral epicondyle (extensor carpi radialis brevis origin), 1 cm distal and slightly anterior to the lateral epicondyle.[11] There is also pain with passive wrist flexion and resistive wrist extension (Cozen's test).[27]
Medical imaging[]
X-rays can confirm and distinguish possibilities of existing causes of pain that are unrelated to tennis elbow, such as fracture or arthritis. Rarely, calcification can be found where the extensor muscles attach to the lateral epicondyle.[11] Medical ultrasonography and magnetic resonance imaging (MRI) are other valuable tools for diagnosis but are frequently avoided due to the high cost.[13] MRI screening can confirm excess fluid and swelling in the affected region in the elbow, such as the connecting point between the forearm bone and the extensor carpi radialis brevis muscle.[citation needed]
Prevention[]
Where lateral epicondylitis is caused by playing tennis, another factor of tennis elbow injury is experience and ability. The proportion of players who reported a history of tennis elbow had an increased number of playing years. As for ability, poor technique increases the chance for injury much like any sport. Therefore, an individual must learn proper technique for all aspects of their sport. The competitive level of the athlete also affects the incidence of tennis elbow. Class A and B players had a significantly higher rate of tennis elbow occurrence compared to class C and novice players. However, an opposite, but not statistically significant, trend is observed for the recurrence of previous cases, with an increasingly higher rate as ability level decreases.[13]
Other ways to prevent tennis elbow:
- Decrease the amount of playing time if already injured or feeling pain in outside part of the elbow.
- Stay in overall good physical shape.
- Strengthen the muscles of the forearm: (pronator quadratus, pronator teres, supinator muscle) and Extensor Carpi Radialis Longus and Brevis[28]—the upper arm: (biceps, triceps)—and the shoulder (deltoid muscle) and upper back (trapezius). Increased muscular strength increases stability of joints such as the elbow.
- Like other sports, use equipment appropriate to your ability, body size, and muscular strength.[13]
- Avoid any repetitive lifting or pulling of heavy objects (especially over your head)[29]
Vibration dampers (otherwise known as "gummies") are not believed to be a reliable preventative measure. Rather, proper weight distribution in the racket is thought to be a more viable option in negating shock.[30]
Treatment[]
Evidence for the treatment of lateral epicondylitis before 2010 was poor.[31] There were clinical trials addressing many proposed treatments, but the trials were of poor quality.[32]
In some cases, severity of tennis elbow symptoms mend without any treatment, within six to 24 months. Tennis elbow left untreated can lead to chronic pain that degrades quality of daily living.[13]
Physical therapy[]
There are several recommendations regarding prevention, treatment, and avoidance of recurrence that are largely speculative including stretches and progressive strengthening exercises to prevent re-irritation of the tendon[33] and other exercise measures.[34]
One way to help treat minor cases of tennis elbow is simply to relax the affected arm. The rest lets stress and tightness within the forearm slowly relax and eventually have the arm in working condition—in a day or two, depending on the case.[citation needed]
Eccentric exercise using a rubber bar is highly effective at eliminating pain and increasing strength.[35][36] The exercise involves grasping a rubber bar, twisting it, then slowly untwisting it.[35][37] Although it can be considered an evidence-based practice, long-term results have not yet been determined.[38]
There are differences in opinions on whether it is okay if pain occurs during these exercises.[39] Some suggest pain of less than 5/10 is okay.[39]
Moderate evidence exists demonstrating that joint manipulation directed at the elbow and wrist and spinal manipulation directed at the cervical and thoracic spinal regions results in clinical changes to pain and function.[40][41] There is also moderate evidence for short-term and mid-term effectiveness of cervical and thoracic spine manipulation as an add-on therapy to concentric and eccentric stretching plus mobilisation of wrist and forearm. Although not yet conclusive, the short-term analgesic effect of manipulation techniques may allow more vigorous stretching and strengthening exercises, resulting in a better and faster recovery process of the affected tendon in lateral epicondylitis.[42]
Low level laser therapy, administered at specific doses and wavelengths directly to the lateral elbow tendon insertions, may result in short-term pain relief and less disability.[43]
Extracorporeal shockwave therapy, while safe, is of unclear benefit.[44][45]
Orthotic devices[]


Orthosis is a device externally used on the limb to improve the function or reduce the pain. Orthotics may be useful in tennis elbow, however long-term effects are unknown.[46] There are two main types of orthoses prescribed for this problem: counterforce elbow orthoses and wrist extension orthoses. Counterforce orthosis has a circumferential structure surrounding the arm. This orthosis usually has a strap which applies a binding force over the origin of the wrist extensors. The applied force by orthosis reduces the elongation within the musculotendinous fibers. Wrist extensor orthosis maintains the wrist in the slight extension. This position reduces the overloading strain at the lesion area.[citation needed]
Studies indicated both type of orthoses improve the hand function[47] and reduce the pain[48] in people with tennis elbow.
Medication[]
Although anti-inflammatories are a commonly prescribed treatment for tennis elbow, the evidence for their effect is usually anecdotal with only limited studies showing a benefit.[49] A systematic review found that topical non-steroidal anti-inflammatory drugs (NSAIDs) may improve pain in the short term (up to 4 weeks) but was unable to draw firm conclusions due to methodological issues.[50] Evidence for oral NSAIDs is mixed.[50]
Evidence is poor for long term improvement from injections of any type, whether corticosteroids, botulinum toxin, prolotherapy or other substances.[51] Corticosteroid injection may be effective in the short term[52] however are of little benefit after a year, compared to a wait-and-see approach.[53] A recent randomized control trial comparing the effect of corticosteroid injection, physiotherapy, or a combination of corticosteroid injection and physiotherapy found that patients treated with corticosteroid injection versus placebo had lower complete recovery or improvement at 1 year (Relative risk 0.86). Patients that received corticosteroid injection also had a higher recurrence rate at 1 year versus placebo (54% versus 12%, relative risk 0.23).[54] Complications from repeated steroid injections include skin problems such as hypopigmentation and fat atrophy leading to indentation of the skin around the injection site.[52] Steroid injections against appear to be more effective than shock wave therapy.[55] Botulinum toxin type A to paralyze the forearm extensor muscles in those with chronic tennis elbow that has not improved with conservative measures may be viable.[56]
Surgery[]
In recalcitrant cases surgery may be an option.[57][58][59] Surgical methods include:[60]
- Lengthening, release, debridement, or repair of the origin of the extrinsic extensor muscles of the hand at the lateral epicondyle
- Rotation of the anconeus muscle
- Denervation of the lateral epicondyle
- Decompression of the posterior interosseous nerve
Surgical techniques for lateral epicondylitis can be done by open surgery, or arthroscopic surgery, with no high-quality evidence that any particular type is better or worse than another.[61][58] Side effects include infection, damage to nerves and inability to straighten the arm.[62] A review of the evidence related to surgery found that published studies were of low quality and did not show that surgery was any more effective than other treatments.[61] A subsequent research trial showed that surgery was no more effective than sham surgery, where patients only received a skin incision, although the trial was limited by a small number of patients.[63]
Prognosis[]
Response to initial therapy is common, but so is relapse (25% to 50%) and/or prolonged, moderate discomfort (40%).[citation needed]
Depending upon severity and quantity of multiple tendon injuries that have built up, the extensor carpi radialis brevis may not be fully healed by conservative treatment. Nirschl defines four stages of lateral epicondylitis, showing the introduction of permanent damage beginning at Stage 2.
- Inflammatory changes that are reversible
- Nonreversible pathologic changes to origin of the extensor carpi radialis brevis muscle
- Rupture of ECRB muscle origin
- Secondary changes such as fibrosis or calcification.[64]
Epidemiology[]
In tennis players, about 39.7% have reported current or previous problems with their elbow. Less than one quarter (24%) of these athletes under the age of 50 reported that the tennis elbow symptoms were "severe" and "disabling," while 42% over the age of 50 did. More women (36%) than men (24%) considered their symptoms severe and disabling. Tennis elbow is more prevalent in individuals over 40, where there is about a four-fold increase among men and two-fold increase among women. Tennis elbow equally affects both sexes and, although men have a marginally higher overall prevalence rate as compared to women, this is not consistent within each age group, nor is it a statistically significant difference.[65]
Playing time is a significant factor in tennis elbow occurrence, with increased incidence with increased playing time being greater for respondents under 40. Individuals over 40 who played over two hours doubled their chance of injury. Those under 40 increased it 3.5 fold compared to those who played less than two hours per day.[13]
History[]
German physician F. Runge[66] is usually credited for the first description of the condition, calling it "writer's cramp" (Schreibekrampf) in 1873.[67] Later, it was called "washer women's elbow".[68] British surgeon Henry Morris published an article in The Lancet describing "lawn tennis arm" in 1883.[69][70] The popular term "tennis elbow" first appeared the same year in a paper by H. P. Major, described as "lawn-tennis elbow".[71][72]
See also[]
References[]
- ^ Jump up to: a b c d e f g h i j k l Hubbard, MJ; Hildebrand, BA; Battafarano, MM; Battafarano, DF (June 2018). "Common Soft Tissue Musculoskeletal Pain Disorders". Primary Care. 45 (2): 289–303. doi:10.1016/j.pop.2018.02.006. PMID 29759125.
- ^ Jump up to: a b c d e f g h i j k "Tennis Elbow (Lateral Epicondylitis)". OrthoInfo. July 2015. Retrieved 21 June 2018.
- ^ Jump up to: a b c d e f g Vaquero-Picado, A; Barco, R; Antuña, SA (November 2016). "Lateral epicondylitis of the elbow". EFORT Open Reviews. 1 (11): 391–397. doi:10.1302/2058-5241.1.000049. PMC 5367546. PMID 28461918.
- ^ Orchard, J; Kountouris, A (10 May 2011). "The management of tennis elbow". BMJ (Clinical Research Ed.). 342: d2687. doi:10.1136/bmj.d2687. PMID 21558359. S2CID 8358075.
- ^ Olaussen, Morten; Holmedal, Øystein; Mdala, Ibrahimu; Brage, Søren; Lindbæk, Morten (2015-05-20). "Corticosteroid or placebo injection combined with deep transverse friction massage, Mills manipulation, stretching and eccentric exercise for acute lateral epicondylitis: a randomised, controlled trial". BMC Musculoskeletal Disorders. 16 (1): 122. doi:10.1186/s12891-015-0582-6. ISSN 1471-2474. PMC 4438532. PMID 25989985.
- ^ Bisset, Leanne; Beller, Elaine; Jull, Gwendolen; Brooks, Peter; Darnell, Ross; Vicenzino, Bill (2006-11-02). "Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial". BMJ. 333 (7575): 939. doi:10.1136/bmj.38961.584653.AE. ISSN 0959-8138. PMC 1633771. PMID 17012266.
- ^ Coombes, Brooke K.; Bisset, Leanne; Brooks, Peter; Khan, Asad; Vicenzino, Bill (2013-02-06). "Effect of Corticosteroid Injection, Physiotherapy, or Both on Clinical Outcomes in Patients With Unilateral Lateral Epicondylalgia: A Randomized Controlled Trial". JAMA. 309 (5): 461–9. doi:10.1001/jama.2013.129. ISSN 0098-7484. PMID 23385272.
- ^ Orchard, JW; Vicenzino, B (20 November 2017). "Cortisone injections for tennis elbow should be an "avoid", rather than a recommended procedure". The Medical Journal of Australia. 207 (10): 453. doi:10.5694/mja17.00445. PMID 29129178. S2CID 20903534.
- ^ Jump up to: a b Lian, Jayson; Mohamadi, Amin; Chan, Jimmy J.; Hanna, Phillip; Hemmati, David; Lechtig, Aron; Nazarian, Ara (2018-10-31). "Comparative Efficacy and Safety of Nonsurgical Treatment Options for Enthesopathy of the Extensor Carpi Radialis Brevis: A Systematic Review and Meta-analysis of Randomized Placebo-Controlled Trials". The American Journal of Sports Medicine. 47 (12): 3019–3029. doi:10.1177/0363546518801914. ISSN 1552-3365. PMID 30380334. S2CID 53148287.
- ^ Wolf, Jennifer Moriatis (2015). Tennis Elbow: Clinical Management. Springer. p. 1. ISBN 9781489975348.
- ^ Jump up to: a b c Essentials of musculoskeletal care. Sarwark, John F. Rosemont, Ill.: American Academy of Orthopaedic Surgeons. 2010. ISBN 978-0892035793. OCLC 706805938.CS1 maint: others (link)
- ^ Geoffroy, P.; Yaffe, M. J.; Rohan, I. (January 1994). "Diagnosing and treating lateral epicondylitis". Canadian Family Physician. 40: 73–78. ISSN 0008-350X. PMC 2379994. PMID 8312757.
- ^ Jump up to: a b c d e f "Tennis Elbow – MayoClinic.com." Mayo Clinic Medical Information and Tools for Healthy Living – MayoClinic.com. 15 Oct. 2008. Web. 10 Oct. 2010. [1]
- ^ Jump up to: a b "Tennis elbow (lateral epicondylitis)", Elbow Pain, Cleveland Clinic, 2018. Accessed 23 January 2018.
- ^ Jump up to: a b "Tennis elbow", Mayo Clinic, Aug. 2, 2017. Accessed 23 January 2018.
- ^ Jump up to: a b Craig Smith, "What is tennis elbow?", BBC Sport Academy. Accessed 23 January 2018.
- ^ Jump up to: a b McShane JM, Nazarian LN, Harwood MI (October 2006). "Sonographically guided percutaneous needle tenotomy for treatment of common extensor tendinosis in the elbow". J Ultrasound Med. 25 (10): 1281–9. doi:10.7863/jum.2006.25.10.1281. PMID 16998100. S2CID 22963436.
- ^ Jump up to: a b c du Toit, C; Stieler, M; Saunders, R; Bisset, L; Vicenzino, B (2008). "Diagnostic accuracy of power Doppler ultrasound in patients with chronic tennis elbow". British Journal of Sports Medicine. 42 (11): 572–576. doi:10.1136/bjsm.2007.043901. hdl:10072/22142. ISSN 0306-3674. PMID 18308874. S2CID 3274396.
- ^ Scott, Alex; Squier, Kipling; Alfredson, Hakan; Bahr, Roald; Cook, Jill L; Coombes, Brooke; de Vos, Robert-Jan; Fu, Siu Ngor; Grimaldi, Alison; Lewis, Jeremy S; Maffulli, Nicola (March 2020). "ICON 2019: International Scientific Tendinopathy Symposium Consensus: Clinical Terminology". British Journal of Sports Medicine. 54 (5): 260–262. doi:10.1136/bjsports-2019-100885. ISSN 0306-3674. PMID 31399426. S2CID 199517946.
- ^ Nirschl RP, Ashman ES (2004). "Tennis elbow tendinosis (epicondylitis)". Instr Course Lect. 53: 587–98. PMID 15116648.
- ^ KURPPA, K., WARIS, P. and ROKKANEN, P. Tennis elbow: Lateral elbow pain syndrome. Scand j. work environ. & health 5 (1979): suppl. 3, 15–18. A review of the etiology, occurrence and pathogenesis of "tennis elbow" is presented.
- ^ "Tennis Elbow (Lateral Epicondylitis)". OrthoInfo. July 2015. Retrieved February 20, 2018.
In racquet sports like tennis, improper stroke technique and improper equipment may be risk factors.
- ^ Keijsers, Renée; de Vos, Robert-Jan; Kuijer, P Paul FM; van den Bekerom, Michel PJ; van der Woude, Henk-Jan; Eygendaal, Denise (2018-09-18). "Tennis elbow". Shoulder & Elbow. 11 (5): 384–392. doi:10.1177/1758573218797973. ISSN 1758-5732. PMC 6739751. PMID 31534489.
- ^ Nirschl RP (October 1992). "Elbow tendinosis/tennis elbow". Clin Sports Med. 11 (4): 851–70. doi:10.1016/S0278-5919(20)30489-0. PMID 1423702.
- ^ Zeisig, Eva; Öhberg, Lars; Alfredson, Håkan (2006). "Sclerosing polidocanol injections in chronic painful tennis elbow-promising results in a pilot study". Knee Surgery, Sports Traumatology, Arthroscopy. 14 (11): 1218–1224. doi:10.1007/s00167-006-0156-0. ISSN 0942-2056. PMID 16960741. S2CID 23469092.
- ^ Jump up to: a b Boyer MI, Hastings H (1999). "Lateral tennis elbow: "Is there any science out there?"". Journal of Shoulder and Elbow Surgery. 8 (5): 481–91. doi:10.1016/S1058-2746(99)90081-2. PMID 10543604.
- ^ Tennis elbow from the MedlinePlus Medical Encyclopedia
- ^ Alizadehkhaiyat, Omid; Frostick, Simon P. (2015-12-01). "Electromyographic assessment of forearm muscle function in tennis players with and without Lateral Epicondylitis" (PDF). Journal of Electromyography and Kinesiology. 25 (6): 876–886. doi:10.1016/j.jelekin.2015.10.013. ISSN 1050-6411. PMID 26559462.
- ^ "Tennis Elbow". DoveMed. Retrieved 2016-12-15.
- ^ http://www.racquetresearch.com/sevencri.htm#What Causes Tennis Elbow?
- ^ Bisset L, Paungmali A, Vicenzino B, Beller E (July 2005). "A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia". British Journal of Sports Medicine. 39 (7): 411–22, discussion 411–22. doi:10.1136/bjsm.2004.016170. PMC 1725258. PMID 15976161.
- ^ Cowan J, Lozano-Calderón S, Ring D (August 2007). "Quality of prospective controlled randomized trials. Analysis of trials of treatment for lateral epicondylitis as an example". The Journal of Bone and Joint Surgery. 89 (8): 1693–9. doi:10.2106/JBJS.F.00858. PMID 17671006.
- ^ Stasinopoulos D, Stasinopoulou K, Johnson MI (December 2005). "An exercise programme for the management of lateral elbow tendinopathy". British Journal of Sports Medicine. 39 (12): 944–7. doi:10.1136/bjsm.2005.019836. PMC 1725102. PMID 16306504.
- ^ "Archived copy". Archived from the original on 2015-04-02. Retrieved 2015-03-12.CS1 maint: archived copy as title (link)
- ^ Jump up to: a b Tyler Timothy F.; Thomas Gregory C.; Nicholas Stephen J.; McHuch Malachy P. (2010). "Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epicondylosis:a radomized trial". Journal of Shoulder and Elbow Surgery. 19 (6): 917–922. doi:10.1016/j.jse.2010.04.041. PMID 20579907.
- ^ Reynolds, Gretchen, "Phys Ed:An Easy Fix for Tennis Elbow?", The New York Times, August 25, 2009, 11:54 pm
- ^ [2]
- ^ Page, Phil (September 2010). "A new exercise for tennis elbow that works!". North American Journal of Sports Physical Therapy. 5 (3): 189–193. ISSN 1558-6162. PMC 2971639. PMID 21589674.
- ^ Jump up to: a b Coombes, Brooke K.; Bisset, Leanne; Vicenzino, Bill (November 2015). "Management of Lateral Elbow Tendinopathy: One Size Does Not Fit All". Journal of Orthopaedic & Sports Physical Therapy. 45 (11): 938–949. doi:10.2519/jospt.2015.5841. ISSN 0190-6011. PMID 26381484.
- ^ Vicenzino B, Cleland JA, Bisset L (2007). "Joint Manipulation in the Management of Lateral Epicondylalgia: A Clinical Commentary". Journal of Manual & Manipulative Therapy. 15 (1): 50–56. doi:10.1179/106698107791090132. PMC 2565595. PMID 19066643.
- ^ Herd CR, Meserve BB (2008). "A Systematic Review of the Effectiveness of Manipulative Therapy in Treating Lateral Epicondylalgia". Journal of Manual & Manipulative Therapy. 16 (4): 225–37. doi:10.1179/106698108790818288. PMC 2716156. PMID 19771195.
- ^ Hoogvliet P, Randsdorp MS, Dingemanse R, Koes BW, Huisstede BM (2013). "Does effectiveness of exercise therapy and mobilisation techniques offer guidance for the treatment of lateral and medial epicondylitis? A systematic review". Br J Sports Med. 47 (17): 1112–9. doi:10.1136/bjsports-2012-091990. PMID 23709519. S2CID 1679092.
- ^ Bjordal JM, Lopes-Martins RA, Joensen J, Couppe C, Ljunggren AE, Stergioulas A, Johnson MI (2008). "A systematic review with procedural assessments and meta-analysis of Low Level Laser Therapy in lateral elbow tendinopathy (tennis elbow)". BMC Musculoskeletal Disorders. 9: 75. doi:10.1186/1471-2474-9-75. PMC 2442599. PMID 18510742.
- ^ "Extracorporeal shockwave therapy for refractory tennis elbow". Interventional procedures guidance. National Institute for Health and Clinical Excellence. August 2009. IPG313.
- ^ Thiele S, Thiele R, Gerdesmeyer L (2015). "Lateral epicondylitis: This is still a main indication for extracorporeal shockwave therapy". International Journal of Surgery. 24 (Pt B): 165–70. doi:10.1016/j.ijsu.2015.09.034. PMID 26455532.
- ^ Struijs, Peter AA; Smidt, Nynke; Arola, H; van Dijk, C N; Buchbinder, Rachelle; Assendelft, Willem JJ (2002-01-21). "Orthotic devices for the treatment of tennis elbow". Cochrane Database of Systematic Reviews. doi:10.1002/14651858.cd001821. ISSN 1465-1858. PMC 8407516.
- ^ Jafarian FS, Demneh ES, Tyson SF (June 2009). "The immediate effect of orthotic management on grip strength of patients with lateral epicondylosis". J Orthop Sports Phys Ther. 39 (6): 484–9. doi:10.2519/jospt.2009.2988. ISSN 0190-6011. PMID 19487823.
- ^ Sadeghi-Demneh, Ebrahim; Jafarian, Fahimehsadat (2013-01-01). "The Immediate Effects of Orthoses on Pain in People with Lateral Epicondylalgia". Pain Research and Treatment. 2013: 353597. doi:10.1155/2013/353597. PMC 3854508. PMID 24349776.
- ^ Jayanthi, Neeru. "Epicondylitis (tennis and golf elbow)". UpToDate. UpToDate, Inc. Retrieved 17 August 2015.
- ^ Jump up to: a b Pattanittum, P; Turner, T; Green, S; Buchbinder, R (May 31, 2013). "Non-steroidal anti-inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults". The Cochrane Database of Systematic Reviews. 5 (5): CD003686. doi:10.1002/14651858.CD003686.pub2. PMC 7173751. PMID 23728646.
- ^ Krogh, TP; Bartels, EM; Ellingsen, T; Stengaard-Pedersen, K; Buchbinder, R; Fredberg, U; Bliddal, H; Christensen, R (June 2013). "Comparative effectiveness of injection therapies in lateral epicondylitis: a systematic review and network meta-analysis of randomized controlled trials". The American Journal of Sports Medicine. 41 (6): 1435–46. doi:10.1177/0363546512458237. PMID 22972856. S2CID 25355427.
- ^ Jump up to: a b Coombes, BK; Bisset, L; Vicenzino, B (Nov 20, 2010). "Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials" (PDF). Lancet. 376 (9754): 1751–67. doi:10.1016/S0140-6736(10)61160-9. hdl:10072/35812. PMID 20970844. S2CID 45054853.
- ^ Haines T, Stringer B (April 2007). "Corticosteroid injections or physiotherapy were not more effective than "wait-and-see" for tennis elbow at one year". Evidence-Based Medicine. 12 (2): 39. doi:10.1136/ebm.12.2.39. PMID 17400631. S2CID 43254510.
- ^ Coombes, BK; Bisset, L; Brooks, P; Khan, A; Vicenzino, B (Feb 6, 2013). "Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondylalgia: a randomized controlled trial" (PDF). JAMA: The Journal of the American Medical Association. 309 (5): 461–9. doi:10.1001/jama.2013.129. PMID 23385272.
- ^ Buchbinder, Rachelle; Green, Sally; Youd, Joanne M; Assendelft, Willem JJ; Barnsley, Les; Smidt, Nynke (2005-10-19). "Shock wave therapy for lateral elbow pain". Cochrane Database of Systematic Reviews (4): CD003524. doi:10.1002/14651858.cd003524.pub2. ISSN 1465-1858. PMID 16235324.
- ^ Kalichman, L; Bannuru, RR; Severin, M; Harvey, W (June 2011). "Injection of botulinum toxin for treatment of chronic lateral epicondylitis: systematic review and meta-analysis". Seminars in Arthritis and Rheumatism. 40 (6): 532–8. doi:10.1016/j.semarthrit.2010.07.002. PMID 20822798.
- ^ Monto, R (September 2014). "Tennis elbow repair with or without suture anchors: a randomized clinical trial". Techniques in Shoulder and ELbow Surgery. 15 (3): 92–97. doi:10.1097/BTE.0000000000000027. S2CID 58020081.
- ^ Jump up to: a b Lo, MY; Safran, MR (October 2007). "Surgical treatment of lateral epicondylitis: a systematic review". Clinical Orthopaedics and Related Research. 463: 98–106. doi:10.1097/BLO.0b013e3181483dc4. PMID 17632419. S2CID 6954029.
- ^ Solheim E, Hegna J, Øyen J (May 2013). "Arthroscopic versus open tennis elbow release: 3- to 6-year results of a case-control series of 305 elbows". Arthroscopy. 29 (5): 854–9. doi:10.1016/j.arthro.2012.12.012. PMID 23388420.
- ^ Faro, Frances; Wolf, Jennifer Moriatis (2007). "Lateral Epicondylitis: Review and Current Concepts". The Journal of Hand Surgery. 32 (8): 1271–1279. doi:10.1016/j.jhsa.2007.07.019. ISSN 0363-5023. PMID 17923315.
- ^ Jump up to: a b Bateman, Marcus; Littlewood, Chris; Rawson, Beth; Tambe, Amol A. (February 2019). "Surgery for tennis elbow: a systematic review". Shoulder & Elbow. 11 (1): 35–44. doi:10.1177/1758573217745041. ISSN 1758-5732. PMC 6348580. PMID 30719096.
- ^ Buchbinder, Rachelle; Johnston, Renea V; Barnsley, Les; Assendelft, Willem JJ; Bell, Simon N; Smidt, Nynke (2011-03-16). "Surgery for lateral elbow pain". Cochrane Database of Systematic Reviews (3): CD003525. doi:10.1002/14651858.cd003525.pub2. ISSN 1465-1858. PMC 7154580. PMID 21412883.
- ^ Kroslak, Martin; Murrell, George A. C. (2018-03-02). "Surgical Treatment of Lateral Epicondylitis: A Prospective, Randomized, Double-Blinded, Placebo-Controlled Clinical Trial". The American Journal of Sports Medicine. 46 (5): 1106–1113. doi:10.1177/0363546517753385. PMID 29498885. S2CID 4487650.
- ^ Owens, Brett D; Moriatis Wolf, Jennifer; Murphy, Kevin P (2009-11-03). "Lateral Epicondylitis: Workup". eMedicine Orthopedic Surgery. Retrieved 2010-04-19.
- ^ Gruchow William, Pelletier Douglas (1979). "An epidemiologic study of tennis elbow: Incidence, recurrence, and effectiveness of prevention strategies". American Journal of Sports Medicine. 7 (4): 234–238. doi:10.1177/036354657900700405. PMID 474862. S2CID 20360265.
- ^ "Tennis Elbow-Cap". The Lancet. 128 (3301): 1083. 1886. doi:10.1016/s0140-6736(00)49587-5.
- ^ Runge F (1873). "Zur Genese und Behandlung des Schreibekrampfes". Berliner Klin Wochenschr. 10: 245–248.
- ^ Science and Racket Sports Edited by: T. Reilly, M. Hughes and A.Lees. Published by E & FN Spon ISBN 0-419-18500-3.
- ^ Flatt Adrian E (Oct 2008). "Tennis elbow". Proc (Bayl Univ Med Cent). 21 (4): 400–402. doi:10.1080/08998280.2008.11928437. PMC 2566914. PMID 18982084.
- ^ "Tennis Elbow-Cap". The Lancet. 128 (3301): 1083. 1886. doi:10.1016/s0140-6736(00)49587-5.
- ^ Major HP (1883). "Lawn-tennis elbow". BMJ. 2 (1185): 556–558. doi:10.1136/bmj.2.1185.556. PMC 2372911.
- ^ Kaminsky SB, Baker CL; Baker (December 2003). "Lateral epicondylitis of the elbow". Techniques in Hand & Upper Limb Surgery. 7 (4): 179–89. doi:10.1097/00130911-200312000-00009. PMID 16518219. S2CID 128648.
External links[]
- Wilson JJ, Best TM (September 2005). "Common overuse tendon problems: A review and recommendations for treatment". American Family Physician. 72 (5): 811–8. PMID 16156339.
| Classification | |
|---|---|
| External resources |
| Authority control: National libraries |
|---|
- Inflammations
- Overuse injuries
- Tennis terminology
- Sports injuries
- Soft tissue disorders
- Tennis culture