Monocyte
| Monocyte | |
|---|---|
 | |
| Details | |
| System | Immune system |
| Identifiers | |
| MeSH | D009000 |
| TH | H2.00.04.1.02010 |
| FMA | 62864 |
| Anatomical terms of microanatomy | |

Monocytes are a type of leukocyte, or white blood cell. They are the largest type of leukocyte and can differentiate into macrophages and conventional dendritic cells. As a part of the vertebrate innate immune system monocytes also influence the process of adaptive immunity. There are at least three subclasses of monocytes in human blood based on their phenotypic receptors.
Structure[]
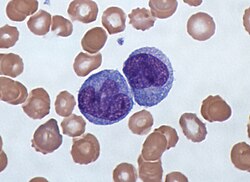
Monocytes are amoeboid in appearance, and have nongranulated cytoplasm.[1] Thus they are classified as agranulocytes. Containing unilobar nuclei, these cells are one of the types of mononuclear leukocytes which shelter azurophil granules. The archetypal geometry of the monocyte nucleus is ellipsoidal; metaphorically bean-shaped or kidney-shaped, although the most significant distinction is that the nuclear envelope should not be hyperbolically furcated into lobes. Contrast to this classification occurs in polymorphonuclear leukocytes. Monocytes compose 2% to 10% of all leukocytes in the human body and serve multiple roles in immune function. Such roles include: replenishing resident macrophages under normal conditions; migration within approximately 8–12 hours in response to inflammation signals from sites of infection in the tissues; and differentiation into macrophages or dendritic cells to effect an immune response. In an adult human, half of the monocytes are stored in the spleen.[2] These change into macrophages after entering into appropriate tissue spaces, and can transform into foam cells in the endothelium.
Subpopulations[]
In humans[]
There are at least three types of monocytes in human blood:[3]
- The classical monocyte is characterized by high level expression of the CD14 cell surface receptor (CD14++ CD16− monocyte)
- The non-classical monocyte shows low level expression of CD14 and additional co-expression of the CD16 receptor (CD14+CD16++ monocyte).[4]
- The intermediate monocyte with high level expression of CD14 and low level expression of CD16 (CD14++CD16+ monocytes).
While in humans the level of CD14 expression can be used to differentiate non-classical and intermediate monocytes, the slan (6-Sulfo LacNAc) cell surface marker was shown to give an unequivocal separation of the two cell types.[5][6]
Ghattas et al. state that the "intermediate" monocyte population is likely to be a unique subpopulation of monocytes, as opposed to a developmental step, due to their comparatively high expression of surface receptors involved in reparative processes (including vascular endothelial growth factor receptors type 1 and 2, CXCR4, and Tie-2) as well as evidence that the "intermediate" subset is specifically enriched in the bone marrow.[7] After stimulation with microbial products the CD14+CD16++ monocytes produce high amounts of pro-inflammatory cytokines like tumor necrosis factor and interleukin-12.
Said et al. showed that activated monocytes express high levels of PD-1 which might explain the higher expression of PD-1 in CD14+CD16++ monocytes as compared to CD14++CD16− monocytes. Triggering monocytes-expressed PD-1 by its ligand PD-L1 induces IL-10 production which activates CD4 Th2 cells and inhibits CD4 Th1 cell function.[8]
In humans a monocyte crawling behavior, similar to the patrolling in mice, has been demonstrated both for the classical and the non-classical monocytes.[9][clarification needed]
In mice[]
In mice, monocytes can be divided in two subpopulations. Inflammatory monocytes (CX3CR1low, CCR2pos, Ly6Chigh, PD-L1neg), which are equivalent to human classical CD14++ CD16− monocytes and resident monocytes (CX3CR1high, CCR2neg, Ly6Clow, PD-L1pos), which are equivalent to human non-classical CD14+ CD16+ monocytes. Resident monocytes have the ability to patrol along the endothelium wall in the steady state and under inflammatory conditions.[10][11][12][13]
Development[]
Monocytes are produced by the bone marrow from precursors called monoblasts, bipotent cells that differentiated from hematopoietic stem cells. Monocytes circulate in the bloodstream for about one to three days and then typically move into tissues throughout the body where they differentiate into macrophages and dendritic cells. They constitute between three and eight percent of the leukocytes in the blood. About half of the body's monocytes are stored as a reserve in the spleen in clusters in the red pulp's Cords of Billroth.[2] Moreover, monocytes are the largest corpuscle in blood.[14]
Macrophages[]
Macrophages are responsible for protecting tissues from foreign substances, but are also suspected to be important in the formation of important organs like the heart and brain. They are cells that possess a large smooth nucleus, a large area of cytoplasm, and many internal vesicles for processing foreign material.
Dendritic cells[]
In vitro, monocytes can differentiate into dendritic cells by adding the cytokines granulocyte macrophage colony-stimulating factor (GM-CSF) and interleukin 4.[15] Such monocyte-derived cells do, however, retain the signature of monocytes in their transcriptome and they cluster with monocytes and not with bona fide dendritic cells.[16]
Function[]
Monocytes and their macrophage and dendritic cell progeny serve three main functions in the immune system. These are phagocytosis, antigen presentation, and cytokine production. Phagocytosis is the process of uptake of microbes and particles followed by digestion and destruction of this material. Monocytes can perform phagocytosis using intermediary (opsonising) proteins such as antibodies or complement that coat the pathogen, as well as by binding to the microbe directly via pattern-recognition receptors that recognize pathogens. Monocytes are also capable of killing infected host cells via antibody-dependent cell-mediated cytotoxicity. Vacuolization may be present in a cell that has recently phagocytized foreign matter.
Many factors produced by other cells can regulate the chemotaxis and other functions of monocytes. These factors include most particularly chemokines such as monocyte chemotactic protein-1 (CCL2) and monocyte chemotactic protein-3 (CCL7); certain arachidonic acid metabolites such as Leukotriene B4 and members of the 5-Hydroxyicosatetraenoic acid and 5-oxo-eicosatetraenoic acid family of OXE1 receptor agonists (e.g., 5-HETE and 5-oxo-ETE); and N-Formylmethionine leucyl-phenylalanine and other N-formylated oligopeptides which are made by bacteria and activate the formyl peptide receptor 1.[17]
Microbial fragments that remain after such digestion can serve as antigens. The fragments can be incorporated into MHC molecules and then trafficked to the cell surface of monocytes (and macrophages and dendritic cells). This process is called antigen presentation and it leads to activation of T lymphocytes, which then mount a specific immune response against the antigen.
Other microbial products can directly activate monocytes and this leads to production of pro-inflammatory and, with some delay, of anti-inflammatory cytokines. Typical cytokines produced by monocytes are TNF, IL-1, and IL-12.
Monocytic cells may contribute to the severity and disease progression in Covid-19 patients.[18]
Clinical significance[]

A monocyte count is part of a complete blood count and is expressed either as a percentage of monocytes among all white blood cells or as absolute numbers. Both may be useful but these cells became valid diagnostic tools only when monocyte subsets are determined.
Monocytosis[]
Monocytosis is the state of excess monocytes in the peripheral blood. It may be indicative of various disease states. Examples of processes that can increase a monocyte count include:
- chronic inflammation
- diabetes[19]
- stress response[20]
- Cushing's syndrome (hyperadrenocorticism)
- immune-mediated disease
- granulomatous disease
- atherosclerosis[21]
- necrosis
- red blood cell regeneration
- viral fever
- sarcoidosis
- chronic myelomonocytic leukemia (CMML)
A high count of CD14+CD16++ monocytes is found in severe infection (sepsis)[22]
In the field of atherosclerosis high numbers of the CD14++CD16+ intermediate monocytes were shown to be predictive of cardiovascular events in at risk populations.[23][24]
CMML patients are characterized by a persistent monocyte count of > 1000/ microL of blood. Analysis of monocyte subsets has demonstrated predominance of classical monocytes and absence of CD14lowCD16+ monocytes.[25][26]
The absence of non-classical monocytes can assist in diagnosis of the disease and the use of slan as a marker can improve specificity.[27]
Monocytopenia[]
Monocytopenia is a form of leukopenia associated with a deficiency of monocytes. A very low count of these cells is found after therapy with immuno-suppressive glucocorticoids.[28]
Also, non-classical slan+ monocytes are strongly reduced in patients with Hereditary diffuse leukoencephalopathy with spheroids (HDLS), a neurologic disease associated with mutations in the macrophage colony-stimulating factor receptor gene.[5]
Blood content[]

See also[]
- Complete blood count
- Hematopoiesis
- Lymphocyte
- Neutrophil granulocyte
- Phagocyte
References[]
- ^ Nichols, Barbara A.; Bainton, Dorothy Ford; Farquhar, Marilyn G. (1 August 1971). "Differentiation of monocytes". Journal of Cell Biology. 50 (2): 498–515. doi:10.1083/jcb.50.2.498. PMC 2108281. PMID 4107019.
- ^ Jump up to: a b Swirski, Filip K.; Nahrendorf, Matthias; Etzrodt, Martin; Wildgruber, Moritz; Cortez-Retamozo, Virna; Panizzi, Peter; Figueiredo, Jose-Luiz; Kohler, Rainer H.; Chudnovskiy, Aleksey; Waterman, Peter; Aikawa, Elena; Mempel, Thorsten R.; Libby, Peter; Weissleder, Ralph; Pittet, Mikael J. (31 July 2009). "Identification of Splenic Reservoir Monocytes and Their Deployment to Inflammatory Sites". Science. 325 (5940): 612–616. Bibcode:2009Sci...325..612S. doi:10.1126/science.1175202. PMC 2803111. PMID 19644120.
- ^ Ziegler-Heitbrock, Loems; Ancuta, Petronela; Crowe, Suzanne; Dalod, Marc; Grau, Veronika; Hart, Derek N.; Leenen, Pieter J. M.; Liu, Yong-Jun; MacPherson, Gordon; Randolph, Gwendalyn J.; Scherberich, Juergen; Schmitz, Juergen; Shortman, Ken; Sozzani, Silvano; Strobl, Herbert; Zembala, Marek; Austyn, Jonathan M.; Lutz, Manfred B. (21 October 2010). "Nomenclature of monocytes and dendritic cells in blood". Blood. 116 (16): e74–e80. doi:10.1182/blood-2010-02-258558. hdl:11379/41075. PMID 20628149.
- ^ Ziegler-Heitbrock, Loems (March 2007). "The CD14+ CD16+ blood monocytes: their role in infection and inflammation". Journal of Leukocyte Biology. 81 (3): 584–592. doi:10.1189/jlb.0806510. PMID 17135573. S2CID 31534841.
- ^ Jump up to: a b Hofer, Thomas P.; Zawada, Adam M.; Frankenberger, Marion; Skokann, Kerstin; Satzl, Anna A.; Gesierich, Wolfgang; Schuberth, Madeleine; Levin, Johannes; Danek, Adrian; Rotter, Björn; Heine, Gunnar H.; Ziegler-Heitbrock, Loems (10 December 2015). "slan-defined subsets of CD16-positive monocytes: impact of granulomatous inflammation and M-CSF receptor mutation". Blood. 126 (24): 2601–2610. doi:10.1182/blood-2015-06-651331. PMID 26443621.
- ^ Hofer, Thomas P.; van de Loosdrecht, Arjan A.; Stahl-Hennig, Christiane; Cassatella, Marco A.; Ziegler-Heitbrock, Loems (13 September 2019). "6-Sulfo LacNAc (Slan) as a Marker for Non-classical Monocytes". Frontiers in Immunology. 10: 2052. doi:10.3389/fimmu.2019.02052. PMC 6753898. PMID 31572354.
- ^ Ghattas, Angie; Griffiths, Helen R.; Devitt, Andrew; Lip, Gregory Y.H.; Shantsila, Eduard (October 2013). "Monocytes in Coronary Artery Disease and Atherosclerosis". Journal of the American College of Cardiology. 62 (17): 1541–1551. doi:10.1016/j.jacc.2013.07.043. PMID 23973684.
- ^ Said, Elias A; Dupuy, Franck P; Trautmann, Lydie; Zhang, Yuwei; Shi, Yu; El-Far, Mohamed; Hill, Brenna J; Noto, Alessandra; Ancuta, Petronela; Peretz, Yoav; Fonseca, Simone G; Van Grevenynghe, Julien; Boulassel, Mohamed R; Bruneau, Julie; Shoukry, Naglaa H; Routy, Jean-Pierre; Douek, Daniel C; Haddad, Elias K; Sekaly, Rafick-Pierre (April 2010). "Programmed death-1–induced interleukin-10 production by monocytes impairs CD4+ T cell activation during HIV infection". Nature Medicine. 16 (4): 452–459. doi:10.1038/nm.2106. PMC 4229134. PMID 20208540.
- ^ Collison, Joanna L.; Carlin, Leo M.; Eichmann, Martin; Geissmann, Frederic; Peakman, Mark (1 August 2015). "Heterogeneity in the Locomotory Behavior of Human Monocyte Subsets over Human Vascular Endothelium In Vitro". The Journal of Immunology. 195 (3): 1162–1170. doi:10.4049/jimmunol.1401806. PMID 26085686.
- ^ Carlin, Leo M.; Stamatiades, Efstathios G.; Auffray, Cedric; Hanna, Richard N.; Glover, Leanne; Vizcay-Barrena, Gema; Hedrick, Catherine C.; Cook, H. Terence; Diebold, Sandra; Geissmann, Frederic (April 2013). "Nr4a1-Dependent Ly6Clow Monocytes Monitor Endothelial Cells and Orchestrate Their Disposal". Cell. 153 (2): 362–375. doi:10.1016/j.cell.2013.03.010. PMC 3898614. PMID 23582326.
- ^ Auffray, Cedric; Fogg, Darin; Garfa, Meriem; Elain, Gaelle; Join-Lambert, Olivier; Kayal, Samer; Sarnacki, Sabine; Cumano, Ana; Lauvau, Gregoire; Geissmann, Frederic (3 August 2007). "Monitoring of Blood Vessels and Tissues by a Population of Monocytes with Patrolling Behavior". Science. 317 (5838): 666–670. Bibcode:2007Sci...317..666A. doi:10.1126/science.1142883. PMID 17673663. S2CID 46067303.
- ^ Imhof, Beat A.; Jemelin, Stephane; Ballet, Romain; Vesin, Christian; Schapira, Marc; Karaca, Melis; Emre, Yalin (16 August 2016). "CCN1/CYR61-mediated meticulous patrolling by Ly6C low monocytes fuels vascular inflammation". Proceedings of the National Academy of Sciences. 113 (33): E4847–E4856. doi:10.1073/pnas.1607710113. PMC 4995973. PMID 27482114.
- ^ Bianchini, Mariaelvy; Duchêne, Johan; Santovito, Donato; Schloss, Maximilian J.; Evrard, Maximilien; Winkels, Holger; Aslani, Maria; Mohanta, Sarajo K.; Horckmans, Michael; Blanchet, Xavier; Lacy, Michael; von Hundelshausen, Philipp; Atzler, Dorothee; Habenicht, Andreas; Gerdes, Norbert; Pelisek, Jaroslav; Ng, Lai Guan; Steffens, Sabine; Weber, Christian; Megens, Remco T. A. (21 June 2019). "PD-L1 expression on nonclassical monocytes reveals their origin and immunoregulatory function". Science Immunology. 4 (36): eaar3054. doi:10.1126/sciimmunol.aar3054. PMID 31227596. S2CID 195259881.
- ^ Steve, Paxton; Michelle, Peckham; Adele, Knibbs (28 April 2018). "The Leeds Histology Guide". leeds.ac.uk. Archived from the original on 11 October 2017. Retrieved 28 April 2018.
- ^ Sallusto, F; Cella, M; Danieli, C; Lanzavecchia, A (1 August 1995). "Dendritic cells use macropinocytosis and the mannose receptor to concentrate macromolecules in the major histocompatibility complex class II compartment: downregulation by cytokines and bacterial products". Journal of Experimental Medicine. 182 (2): 389–400. doi:10.1084/jem.182.2.389. PMC 2192110. PMID 7629501.
- ^ Robbins, Scott H; Walzer, Thierry; Dembélé, Doulaye; Thibault, Christelle; Defays, Axel; Bessou, Gilles; Xu, Huichun; Vivier, Eric; Sellars, MacLean; Pierre, Philippe; Sharp, Franck R; Chan, Susan; Kastner, Philippe; Dalod, Marc (2008). "Novel insights into the relationships between dendritic cell subsets in human and mouse revealed by genome-wide expression profiling". Genome Biology. 9 (1): R17. doi:10.1186/gb-2008-9-1-r17. PMC 2395256. PMID 18218067.
- ^ Sozzani, S.; Zhou, D.; Locati, M.; Bernasconi, S.; Luini, W.; Mantovani, A.; O'Flaherty, J. T. (15 November 1996). "Stimulating properties of 5-oxo-eicosanoids for human monocytes: synergism with monocyte chemotactic protein-1 and -3". The Journal of Immunology. 157 (10): 4664–4671. PMID 8906847.
- ^ Gómez-Rial, Jose; Rivero-Calle, Irene; Salas, Antonio; Martinón-Torres, Federico (22 July 2020). "Role of Monocytes/Macrophages in Covid-19 Pathogenesis: Implications for Therapy". Infection and Drug Resistance. 13: 2485–2493. doi:10.2147/IDR.S258639. PMC 7383015. PMID 32801787.
- ^ Hoyer, FF; Zhang, X; Coppin, E; Vasamsetti, SB; Modugu, G; Schloss, MJ; Rohde, D; McAlpine, CS; Iwamoto, Y; Libby, P; Naxerova, K; Swirski, F; Dutta, P; Nahrendorf, P (April 2020). "Bone Marrow Endothelial Cells Regulate Myelopoiesis in Diabetes". Circulation. 142 (3): 244–258. doi:10.1161/CIRCULATIONAHA.120.046038. PMC 7375017. PMID 32316750.
- ^ Heidt, Timo; Sager, Hendrik B; Courties, Gabriel; Dutta, Partha; Iwamoto, Yoshiko; Zaltsman, Alex; von zur Muhlen, Constantin; Bode, Christoph; Fricchione, Gregory L; Denninger, John; Lin, Charles P; Vinegoni, Claudio; Libby, Peter; Swirski, Filip K; Weissleder, Ralph; Nahrendorf, Matthias (July 2014). "Chronic variable stress activates hematopoietic stem cells". Nature Medicine. 20 (7): 754–758. doi:10.1038/nm.3589. PMC 4087061. PMID 24952646.
- ^ Swirski, Filip K.; Libby, Peter; Aikawa, Elena; Alcaide, Pilar; Luscinskas, F. William; Weissleder, Ralph; Pittet, Mikael J. (2 January 2007). "Ly-6Chi monocytes dominate hypercholesterolemia-associated monocytosis and give rise to macrophages in atheromata". Journal of Clinical Investigation. 117 (1): 195–205. doi:10.1172/JCI29950. PMC 1716211. PMID 17200719.
- ^ Fingerle, G; Pforte, A; Passlick, B; Blumenstein, M; Strobel, M; Ziegler- Heitbrock, Hw (15 November 1993). "The novel subset of CD14+/CD16+ blood monocytes is expanded in sepsis patients". Blood. 82 (10): 3170–3176. doi:10.1182/blood.v82.10.3170.3170. PMID 7693040.
- ^ Heine, G.H.; Ulrich, C.; Seibert, E.; Seiler, S.; Marell, J.; Reichart, B.; Krause, M.; Schlitt, A.; Köhler, H.; Girndt, M. (March 2008). "CD14++CD16+ monocytes but not total monocyte numbers predict cardiovascular events in dialysis patients". Kidney International. 73 (5): 622–629. doi:10.1038/sj.ki.5002744. PMID 18160960.
- ^ Rogacev, Kyrill S.; Cremers, Bodo; Zawada, Adam M.; Seiler, Sarah; Binder, Nadine; Ege, Philipp; Große-Dunker, Gunnar; Heisel, Isabel; Hornof, Florian; Jeken, Jana; Rebling, Niko M.; Ulrich, Christof; Scheller, Bruno; Böhm, Michael; Fliser, Danilo; Heine, Gunnar H. (October 2012). "CD14++CD16+ Monocytes Independently Predict Cardiovascular Events". Journal of the American College of Cardiology. 60 (16): 1512–1520. doi:10.1016/j.jacc.2012.07.019. PMID 22999728.
- ^ Vuckovic, S.; Fearnley, D. B.; Gunningham, S.; Spearing, R. L.; Patton, W. N.; Hart, D. N. J. (June 1999). "Dendritic cells in chronic myelomonocytic leukaemia: Dendritic Cells in CMML". British Journal of Haematology. 105 (4): 974–985. doi:10.1046/j.1365-2141.1999.01431.x. PMID 10554809. S2CID 22571555.
- ^ Selimoglu-Buet, Dorothée; Wagner-Ballon, Orianne; Saada, Véronique; Bardet, Valérie; Itzykson, Raphaël; Bencheikh, Laura; Morabito, Margot; Met, Elisabeth; Debord, Camille; Benayoun, Emmanuel; Nloga, Anne-Marie; Fenaux, Pierre; Braun, Thorsten; Willekens, Christophe; Quesnel, Bruno; Adès, Lionel; Fontenay, Michaela; Rameau, Philippe; Droin, Nathalie; Koscielny, Serge; Solary, Eric (4 June 2015). "Characteristic repartition of monocyte subsets as a diagnostic signature of chronic myelomonocytic leukemia". Blood. 125 (23): 3618–3626. doi:10.1182/blood-2015-01-620781. PMC 4497970. PMID 25852055.
- ^ Tarfi, Sihem; Badaoui, Bouchra; Freynet, Nicolas; Morabito, Margot; Lafosse, Jeffie; Toma, Andréa; Etienne, Gabriel; Micol, Jean-Baptiste; Sloma, Ivan; Fenaux, Pierre; Solary, Eric; Selimoglu-Buet, Dorothée; Wagner-Ballon, Orianne (April 2020). "Disappearance of slan-positive non-classical monocytes for diagnosis of chronic myelomonocytic leukemia with an associated inflammatory state". Haematologica. 105 (4): e147–e152. doi:10.3324/haematol.2019.219782. PMID 31413091. S2CID 199663779.
- ^ Fingerle-Rowson, G; Angstwurm, M; Andreesen, R; Ziegler-Heitbrock, HW (June 1998). "Selective depletion of CD14 + CD16 + monocytes by glucocorticoid therapy: Depletion of CD14+ CD16+ monocytes by glucocorticoids". Clinical & Experimental Immunology. 112 (3): 501–506. doi:10.1046/j.1365-2249.1998.00617.x. PMC 1904988. PMID 9649222.
External links[]
- Histology image: 01702ooa – Histology Learning System at Boston University
- Human Monocytes — Prof. Dr. Ziegler-Heitbrock
- Circulation of Body Fluids
| show Authority control |
|---|
- Mononuclear phagocytes
- Immune system
- Cell biology
- Human cells